Editor’s Note: This article is periodically updated with more stats on premature ejaculation as we find and vet them.
Last Updated: January 25, 2023.
Premature ejaculation (PE) is the most common form of sexual dysfunction affecting men. To date, there has been no universally acknowledged definition of premature ejaculation. This has complicated the analysis and examination of the condition in clinical settings. Premature ejaculation statistics vary across geographic and sociocultural settings. The elucidation of premature ejaculation and its risk factors has been difficult.
But then, this condition tends to have several risk factors which are strongly supported by medical findings. To effectively tackle the menace of PE, it is important to have an in-depth understanding of premature ejaculation statistics.
Table of Contents
Premature Ejaculation Statistics
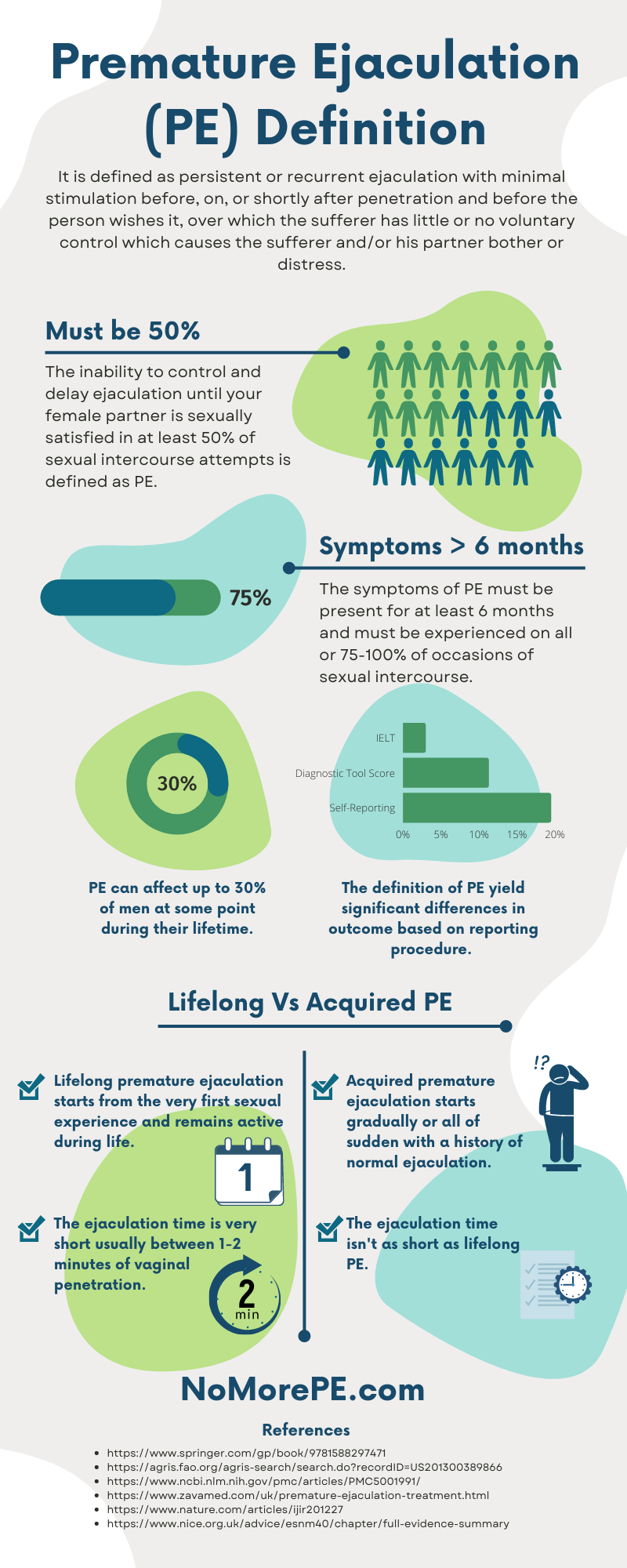
- Premature ejaculation is defined as persistent or recurrent ejaculation with minimal stimulation before, on, or shortly after penetration and before the person wishes it, over which the sufferer has little or no voluntary control which causes the sufferer and/or his partner bother or distress. (WHO)
- The inability to control and delay ejaculation until your female partner is sexually satisfied in at least 50% of sexual intercourse attempts is defined as premature ejaculation. (Masters, 1980)
- The symptoms of premature ejaculation must be present for at least 6 months and must be experienced on all or 75-100% of occasions of sexual intercourse. (DSM-V)
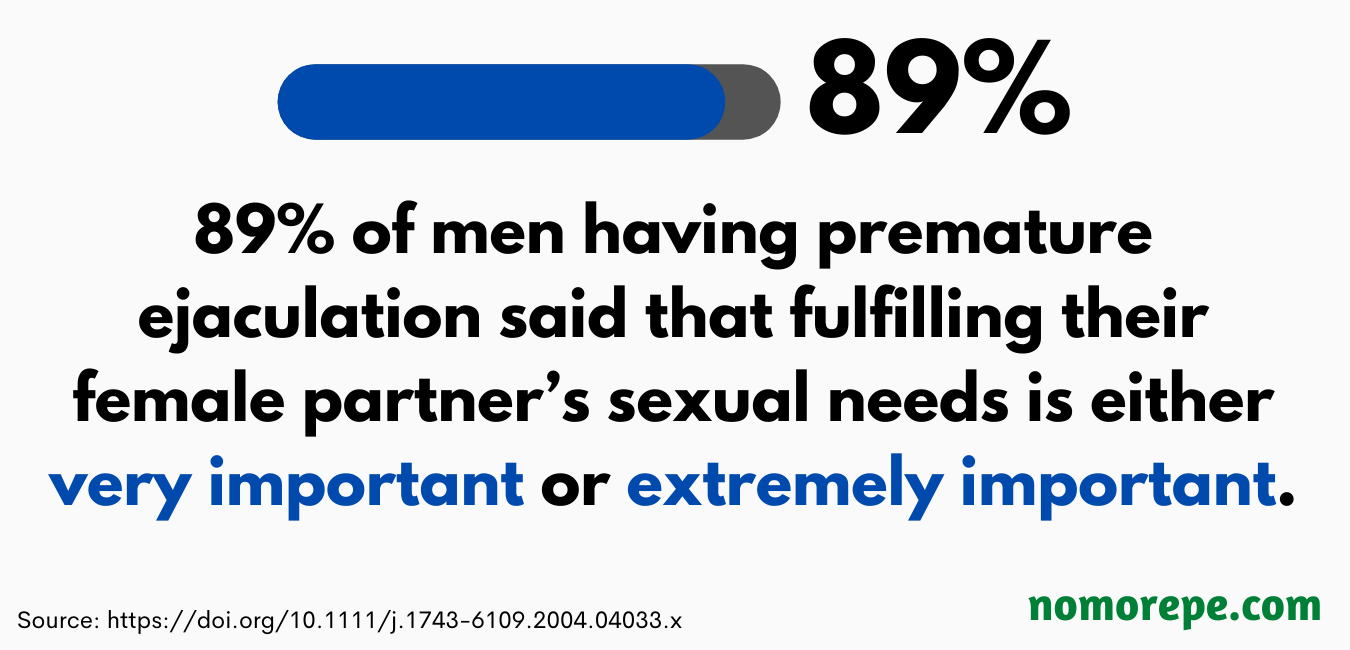
- Over 89% of men having premature ejaculation reported that fulfilling their female partner’s sexual needs and satisfaction is either very important or extremely important. (Rowland, 2008)
- It is one of the most common male sexual disorders estimated to occur in 4-39% of men of all age groups. (Reading, 1984)
- Premature ejaculation can affect up to 30% of men at some point during their lifetime. (Zava)
- A report by the National Institute for Health and Care Excellence found that premature ejaculation affects 20-30% of men globally. (NICE)
- Lifelong premature ejaculation starts from the very first sexual experience and remains active during life and the ejaculation time is very short usually between 1-2 minutes of vaginal penetration. (NICE)
- Acquired premature ejaculation starts gradually or all of sudden with a history of normal ejaculation. The ejaculation time isn’t as short as lifelong PE. (NICE)
- A Korean study found that the definition of premature ejaculation yielded significant differences in outcome. Premature ejaculation had a 19.5% prevalence by self-reporting, 3% based on intravaginal ejaculation latency time recorded by stopwatch, and 11.3% based on a diagnostic tool score of 11 or above. (Lee, 2012)
- Premature ejaculation has a global prevalence of approximately 30%. (Carson, 2006)
- The average length of sex is 7.3 minutes but 43% of men finish in less than 2 minutes. (Psychology Today)
- The average duration of intercourse is 4-7 minutes. (Gebhard, 1966)
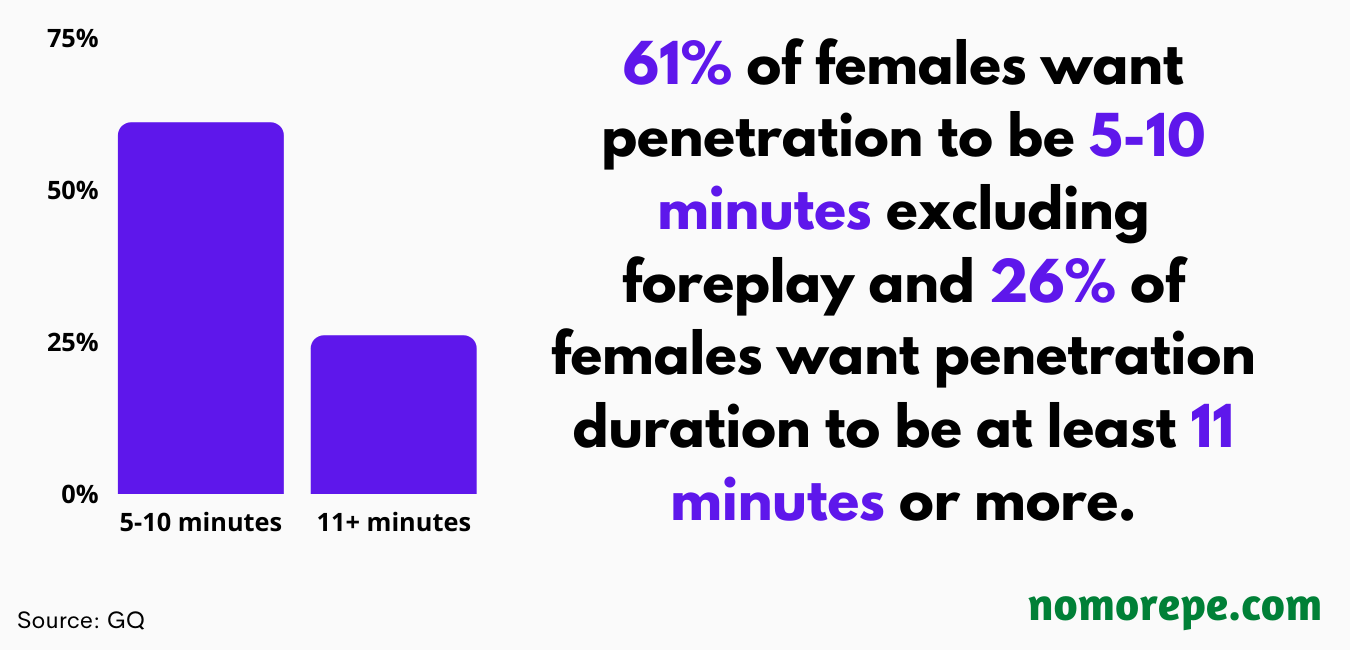
- Sixty-one percent of females want penetration to be 5-10 minutes excluding foreplay and 26% of females want penetration duration to be at least 11 minutes or more. (GQ)
- According to a one-month study of 500 heterosexual couples, the ejaculation time ranged between 33 seconds to 44.1 minutes with an average being 5.4 minutes. (Waldinger, 2005)
- Higher education, divorce, and social phobia are three key factors that increase the risk of premature ejaculation. (Tignol, 2006)
- PE is more common in younger men as compared to older ones. The risk of PE decreases with age. (Basile Fasolo, 2001)
- Ejaculation time of less than a minute is considered severe PE. (Waldinger, 1998)
- Thirty-one percent of men suffering from PE reported sexual satisfaction as poor or very poor. (Patrick, 2005)
- Sixty-four percent of men with PE reported feelings of personal distress. (Patrick, 2005)
- As much as 50% of men who have erectile dysfunction also have premature ejaculation. (Laumann, 2005)
- A study found that 59% of premature ejaculation cases were diagnosed in men of Middle Eastern or Asian descent, while 41% of cases were diagnosed in men of European or Western birth. (Frewen, 2007)
- Rapid ejaculation distress is negatively associated with sexual performance, increases the risk of erectile dysfunction, and leads to depression in the sexual couple. (Corona, 2021)
- There is a higher prevalence (34%) of premature ejaculation among African American men and white men (29%) compared to Hispanic men who had a prevalence of 27%. (Giuliano, 2008)
- Premature ejaculation has a highly variable prevalence and depends on the definition employed. Although 30% of men between the ages of 8-70 report being concerned about how fast they ejaculate, only 1-3% are diagnosed with premature ejaculation according to the DSM-5 criteria. The DSM-5 criteria define premature ejaculation as ejaculation occurring within 60 seconds after penetration and before the individual wishes. (DSM-5)
- Premature ejaculation statistics in India and European countries mirror the statistics in the United States. The prevalence in Africa, Asia, and Australia, and other parts of the world is not known. (Verma, 1998)
Premature Ejaculation Treatment Statistics
- A clinical study found that using sildenafil 50-100 mg for 1-3 months can improve premature ejaculation by 60%. Forty out of 45 patients had erectile improvement by 88.88% and sexual satisfaction was improved by 81.48% in 27 patients. (Li, 2003)
- A study found that vardenafil increases ejaculation duration (IELT) by 9.7 times. (Sommer, 2005)
- Using both sildenafil and vardenafil to cure erectile dysfunction significantly decreases premature ejaculation. (Sommer (2005) and Li (2003))
- Topical 4% benzocaine wipes improve premature ejaculation symptoms significantly and delay ejaculation by 231.5 seconds. (Shabsigh, 2017)
- Benzocaine wipes increase intravaginal ejaculation latency time (IELT) by 2.75 minutes after a month of use and by 5.5 minutes after 2 months of use. (Shabsigh, 2019)
- Lidocaine 5% spray 10-20 minutes before sexual intercourse can significantly increase the frequency of sexual intercourse and intravaginal ejaculatory latency times. (Abu El-Hamd, 2021)
- A mixture of lidocaine and prilocaine spray improves IELT, ejaculatory control, and sex quality by 2.4 times. (Dinsmore, 2007)
- In a 2-months clinical study, patients were given lidocaine-based spray to cure premature ejaculation. And for the next 2-months, all the patients received behavioral therapy with medical treatment being stopped. The results showed that for the first 2-months, subjects had an average increase of ejaculation time by 8x and this reduced to 1.7x during behavioral therapy. This shows that medical treatment is more effective than behavioral techniques. (Steggall, 2008)
- Lidocaine-prilocaine cream 5% increases IELT significantly when applied 20 minutes before intercourse. (Atikeler, 2002)
- A clinical study involving 84 men having PE showed that men who used 45 mg sildenafil 45 minutes before intercourse and applied lidocaine-prilocaine cream on penis 15 minutes before sex showed 86.4% improvement in ejaculation time. (Atan, 2006)
- Applying topical herbal cream on the penis before intercourse increased IELT from 1.37-10.92 minutes and 82% of men were more satisfied with their sexual performance. (Choi, 2000)
- Topical treatments of premature ejaculation are recommended as they perform better than behavioral techniques. (Hatzimouratidis, 2010)
- Paroxetine is the best selective serotonin reuptake inhibitor (SSRI) for premature ejaculation treatment among clomipramine, fluoxetine, and sertraline. (Waldinger 1998, 2001)
- Dapoxetine is found to increase IELT by 2.5-3 minutes and has tolerable side effects. It also absorbs quickly in the skin as compared to other SSRIs. (Pryor, 2006)
- In a clinical study, dapoxetine increased ejaculation time (IELT) from baseline of 0.9 minutes to 3.1 minutes (30 mg) and 3.6 minutes (60 mg) in 12 weeks. (Buvat (2009) and McMahon (2011))
- A double-blind placebo-controlled study found that sildenafil significantly increases confidence, ejaculation control, and sexual satisfaction in men. It also decreased the time to get a second erection after ejaculation. (McMahon, 2005)
- A double-blind parallel-group study found that sildenafil significantly increased IELT and sexual satisfaction in men with PE. It also reduced anxiety and performed better than SSRIs and the pause-squeeze technique. (McMahon and Wang, 2006)
Premature Ejaculation Behavioral Technique Statistics
- A 12-week physical therapy (physio-kinesiotherapy, biofeedback, and electrostimulation of the perineal floor) helped 80% of participants gain control over ejaculation and it improved ejaculation time by at least a minute. (Pastore, 2014)
- The start-stop technique is known to help improve and even stop premature ejaculation in as much as 45-65% of men. (Mohee, 2011)
- Pelvic floor muscle exercises may help improve premature ejaculation and erectile dysfunction. (Myers, 2019)
- Both psychotherapy and medication are more effective at curing premature ejaculation than medication alone. (Althof, 2016)
- Behavioral programs, such as the start-stop technique, are effective as long as they’re used with medical treatment to cure PE. (Carufel, 2006)
- A systematic review found that behavioral techniques such as squeeze method are effective in delaying ejaculation and the effect increases when such techniques are used in combination with other treatment method (e.g., drugs). However, the studies are limited and more evidence is needed on the effectiveness of behavioral techniques in curing PE. (Cooper, 2015)
Time to Take Premature Ejaculation Seriously
It is important to note, though, that most men with this condition do not report it to their healthcare provider. This may be due to low self-esteem, a feeling of embarrassment, or the feeling that there’s no available treatment for the condition. Some men do not even consider premature ejaculation a problem.
It is also worth noting that premature ejaculation is not age-dependent. Clinical research and experience have shown that it can occur at any age in a man’s life. However, it is commonly reported among men aged 18-30 years. It may also occur alongside secondary impotence in men between the ages of 45-65.
Currently, no data is showing significant differences between races concerning the prevalence or incidence of premature ejaculation. But then, a couple of surveys suggest that there may be some degree of racial variation.
Premature ejaculation has a negative impact on the sex life of men and their partners. Men who experience it are not likely to report or seek help for it. As such, acceptance and improved awareness of this condition is of utmost importance to both clinicians and patients. An in-depth understanding of premature ejaculation statistics will improve its clinical management.